
Conference Presentation
Breast Cancer Screening with Digital Breast Tomosynthesis Improves Cancer Detection Across Race, Ethnicity, and Income
RSNA 2022
Leeann D. Louis, Bryan Haslam, Jiye G. Kim, William Lotter, A. Gregory Sorensen
November 30, 2022
Purpose
Breast cancer screening mammography using digital breast tomosynthesis (DBT) is thought to be an improvement over full-field digital mammography (FFDM) leading to increased cancer detection rate (CDR) and reduced recall rate (RR). Although performance has been shown at a population level, less evidence is available that DBT provides an improvement for different patient subgroups, especially for patients with different racial, ethnic or economic backgrounds. The goal of this study was to determine if improvements from DBT are also found across race, ethnicity, and income.
Materials and Method
Retrospective data taken from 2017-2021 was collected from over 200 clinical sites across the United States. Outcomes measured included RR (%), CDR (per 1,000 women screened), interval cancer rate (ICR, per 1,000 women screened), and positive predictive value of recalls (PPV, %). Race and ethnicity were taken from self-reported intake forms. Income was estimated using the median income from each patient’s zip code as tabulated in the 2021 US Census. Analyses were performed by modality (DBT vs. FFDM), as well as race/ethnicity and income. Comparisons were performed using Chi Square tests with FDR correction for multiple tests.
Results
Data included screening mammograms (excluding first screens) from 906,413 women (median age 60.5±10.5 years); at least 1 year of followup was available for all screens. 64% of these exams were DBT. DBT had similar RR (DBT 7.9% vs. FFDM 7.5%), higher CDR (DBT 4.35 vs. FFDM 3.11) and higher PPV (DBT 5.50% vs. FFDM 4.14%). The real strength of the dataset was its coverage of the screening population by race (White n=785,352, Black or African American n=304,296, Asian n=151,267), ethnicity (Hispanic or Latino n=277,147), and income level (<$50k: n=224,355; $50-75k: n=503,773; $75-100k: n=374,179; >$100k: n=410,324). Including these features in the analysis revealed that DBT had significantly higher CDR and PPV for all races, ethnicities, and income levels (p < 0.001 in all groups). ICR did not differ significantly between DBT and FFDM overall or for any racial, ethnic, or income population.
Conclusion
Consistent with prior studies, breast cancer screening with DBT had a higher CDR and PPV compared with FFDM. This performance improvement with DBT was consistent across races, ethnicities, and socioeconomic status.
Clinical Relevance
Screening using DBT improves performance over FFDM regardless of race, ethnicity, or income.
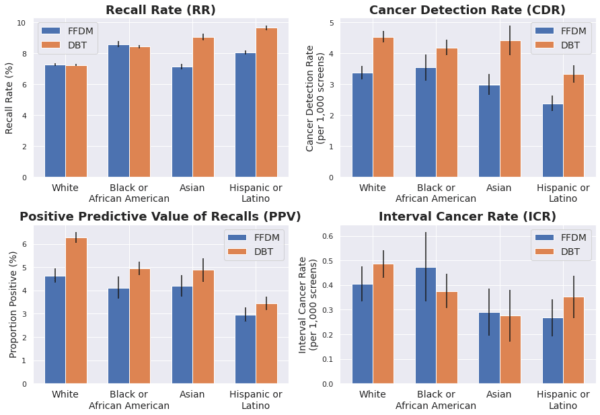
Figure 1.
Screening mammography outcomes analyzed by race / ethnicity and modality.